
“These patients will lose much alveolar bone if we do nothing.”

Thin vs thick biotypes, tooth-root angulation – what are the differences between socket anatomy in Asian and Caucasian patients? And what do these differences mean for implant placement? We talked with three experts from two continents
Dr. Araújo, you are one of the first investigators of the sequence of biological events after tooth extraction. In brief, what happens?
Dr. Araújo: The healing process is divided into three phases: inflammatory, proliferative and modeling/remodeling. In the last phase, the osteoclast activity promotes extensive bone resorption that reduces the alveolar ridge dimension. Facial bony walls are frequently thinner than 1 mm, and these thin walls are almost exclusively bundle bone.1 Because it is a completely tooth-dependent structure, the bundle bone is resorbed after tooth extraction.
How much volume is lost on average? There are so many studies, site-specific factors, measurement points and methods… do you have an easy answer?
Dr. Araújo: On average, in the esthetic zone, about 50 % of the width and 30 % of the volume of the alveolar ridge is lost.2 This amount is very significant. Is the process of bone resorption similar in all patients and sites? Dr. Araújo: The process is the same in all patients, but the clinical outcome is different. A thin buccal bone wall, a narrow alveolar socket and a socket outside the bone envelope may significantly increase the volume loss.
Dr. Yeo, you investigated one of these conditions that affect bone resorption after tooth extraction in more detail: tooth-alveolus angulation. What does this term mean?
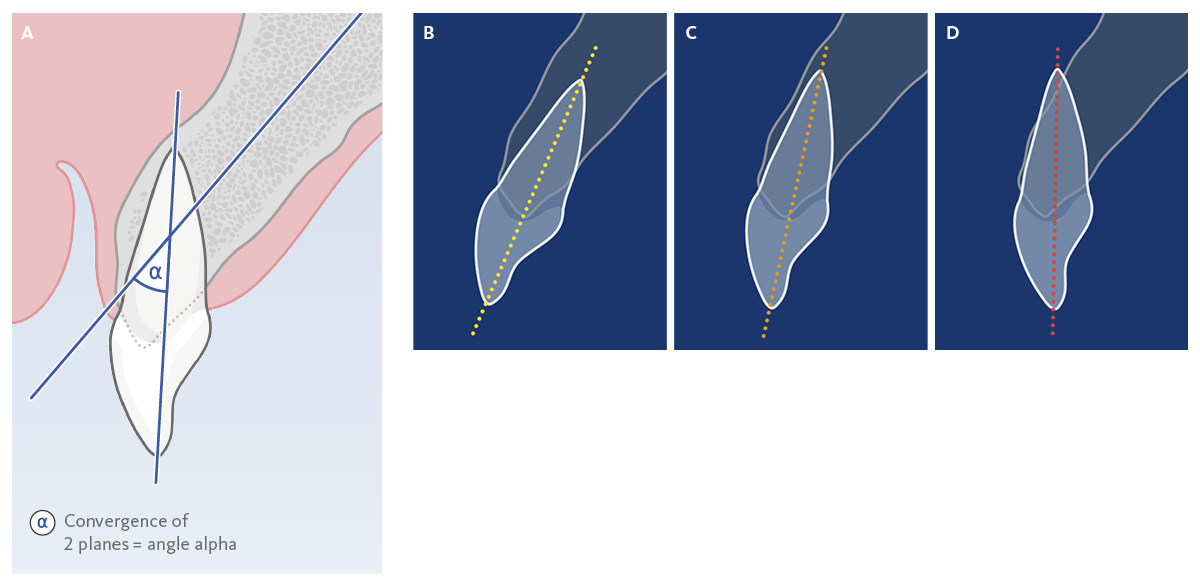
Dr. Yeo: Tooth-alveolus angulation is the angle measured where the axial planes of tooth-root and the alveolus converge (Fig. 1). A small angle suggests that the entire tooth-root is expected to be positioned within the alveolar housing. In case of a large angle, the root will be positioned very close to the buccal bone wall or even out of the buccal aspect of the alveolar housing.
How frequent is this condition?
Dr. Yeo: To the best of my knowledge, we have many reports of angulation issues in Asian populations but limited or none in Caucasians. In a study from China, 50% of the study population (n=300) had tooth-alveolus angulations of more than 20 degrees.3 In our study in Singapore we measured an average tooth-root angulation of 13.6 degrees.4 Almost 36 % of our study population (n=100) had tooth-root angulations of more than 15 degrees.4 Also in my own clinical practice, about 20% have moderate to severe tooth-alveolus angulations.
In case of severely angulated teeth, what are the consequences for bone healing after tooth extraction?
Dr. Yeo: These sockets often already show buccal bone dehiscences, fenestrations or perforations before tooth extraction, leading to significant bone defects after healing. In the publication from Chappius et al in 2013, there was almost seven times more mid-facial bone loss when the original tooth socket presented with a thin and compromised bone phenotype.5
Dr. Iwano, you also investigated the differences between extraction sockets in Asian, especially Japanese, and Caucasian patients. What were your findings?
Dr. Iwano: Compared with the data for Caucasians, it seems that the buccal bone walls of Japanese patients are clearly thinner, especially in the maxillary anterior teeth.6 At 5 mm from the alveolar crest, we have on average 0.24 mm thickness, and at 6 mm only 0.20 mm.6 It is assumed that the alveolar bone thickness is very thin not only in the central part but also in the mesiodistal part of the anterior tooth.
What does this mean for tooth extraction?
Dr. Iwano: The bundle bone is about 0.2 to 0.4 mm thick – just like the reported average bone width.6 So, in the case of Japanese people, we can assume that the alveolar bone in the central part of the labial side will fully resorb after tooth extraction.
Let’s discuss how to deal with these conditions for implant placement. Dr. Yeo, you once said that you had several “oops-moments” when you wanted to perform early implant placement on your patients in Singapore. What caused the “oops”?
Dr. Yeo: Standard and proven protocols for tooth extraction followed by early implant placement somehow did not work out for about twenty percent of my maxillary cases. When opening the flap I realized that implant site preparation and implant placement were not possible. The amount of bone loss and remodeling following tooth extraction was too extensive, so I had to perform a staged-approach GBR instead.
Which is more invasive and costs additional time for the patient...
Dr. Yeo: Yes. Patients are subjected to more treatment morbidity, cost and the overall treatment time is longer.
How do you deal with such cases in your daily practice?
Dr. Yeo: In esthetically and anatomically demanding cases, we routinely take a CBCT image to evaluate the tooth-alveolus angulation profile. Based on this we can decide whether to perform Ridge Preservation following tooth extraction. By doing so we have managed to perform implant placement in most of these cases using a ‘delayed’ early implant placement approach after around twelve to sixteen weeks, instead of a two-stage GBR approach.
So you don’t perform Ridge Preservation to avoid a GBR but to avoid two-stage GBR?
Dr. Yeo: Absolutely. Simultaneous GBR or contour augmentation during implant placement is still required.
Dr. Araújo, how do you see this from an economic perspective? Does Ridge Preservation also “pay off” in these cases? Or is it more of a patient investment in a less invasive treatment?
Dr. Araújo: In Alvin Yeo’s example, Ridge Preservation helps to avoid a two-stage GBR procedure and thereby makes the treatment less invasive. So, perhaps it is not an obvious economical benefit, but it is definitely a way to reduce surgical morbidity. From an economic perspective, Ridge Preservation pays off in cases where it helps to avoid a further GBR procedure. It is important to obtain a CBCT of the alveolar socket before extraction and confirm that it has at least 9 mm of thickness so that, even with minor volume loss after Ridge Preservation, the dimension is sufficient for implant placement. And one needs to check whether the buccal bone is intact or not, etc.
Dr. Iwano, is Ridge Preservation a standard treatment after tooth extraction in Japan?
Dr. Iwano: Not yet. In 2018 we completed a questionnaire with 248 implant dentists, including 103 specialists from the Japanese Society of Oral Implantology. In that questionnaire we asked whether clinicians perform Ridge Preservation when extracting teeth on the premise of implant treatment. 32.3% of the participants said “yes”.7 I am one of those who answered “yes,” because I personally always perform Ridge Preservation and think that it is useful. But the current situation is that it is not yet the standard of treatment in Japan.
In which patients do you support Ridge Preservation? And why?
Dr. Iwano: It is performed for all patients who have thin buccal bone plates, because these patients will lose a considerable amount of alveolar bone if we do nothing. Consequently, they will need large amounts of bone augmentation in case of subsequent implant placement. Ridge Preservation is a simple and minimally invasive surgical procedure that – if performed simultaneously with tooth extraction – will enable implant treatment without the need for large bone augmentations. Bone resorption after tooth extraction also causes problems for bridge restorations. Since esthetic problems and poor cleaning may occur due to the lengthening of the pontic, keeping the amount of resorption of the alveolar ridge to a minimum using Ridge Preservation will bring great benefits.
Short & sweet: what role does soft tissue play?
Dr. Iwano: In patients with thin hard tissues, the presence of thick soft tissue is extremely important for maintaining esthetics. People with thin hard tissue often require soft tissue augmentation.
References
- Januario AL, et al.: Clin Oral Impl Res 2011; 10: 1168–71. (clinical study)
- Misawa M, et al.: Clin Oral Implants Res 2016; 27(7): 884-9. (clinical study)
- Wang HM, et al.: Int J Oral Maxillofac Implants 2014; 29(5): 1123-29. (clinical study)
- Lee WZ, et al.: 2021 – in preparation (clinical study)
- Chappuis V, et al.: J Dent Res. 2013; 92 (12 Suppl): 195S-201S. (clinical study)
- Ezawa T.: J Jpn. Soc Periodontol. 1984; 26: 243-56. (clinical study)
- Iwano Y et al.: The Clinical Question. Tokyo; Quintessence, 2018: 148-149. (book chapter)
About the author

Manager Medical Communications
Geistlich Pharma



