"Nobody wants to hide their smile"

Dr. Frank Bröseler has been practicing periodontal regenerative therapy for 20 years with great success and has investigated what really matters for patients. We spoke to him about goals, expectations and the best time to re-motivate patients.
Dr. Bröseler, you published a retrospective study about periodontal regenerative therapy in a large day-to-day patient population.1 What did you want to find out?
Dr. Bröseler: We were interested in whether the very good results from wellknown, prospective studies2, 3 could be confirmed in a normal practice environment. In prospective studies, selected patients are treated – patients without major health problems, with good compliance, non-smokers, etc. But what is the success of a therapy when treating any Tom, Dick and Harry? For instance, patients who suffer from diabetes or have less than perfect oral hygiene?
And what did you discover?
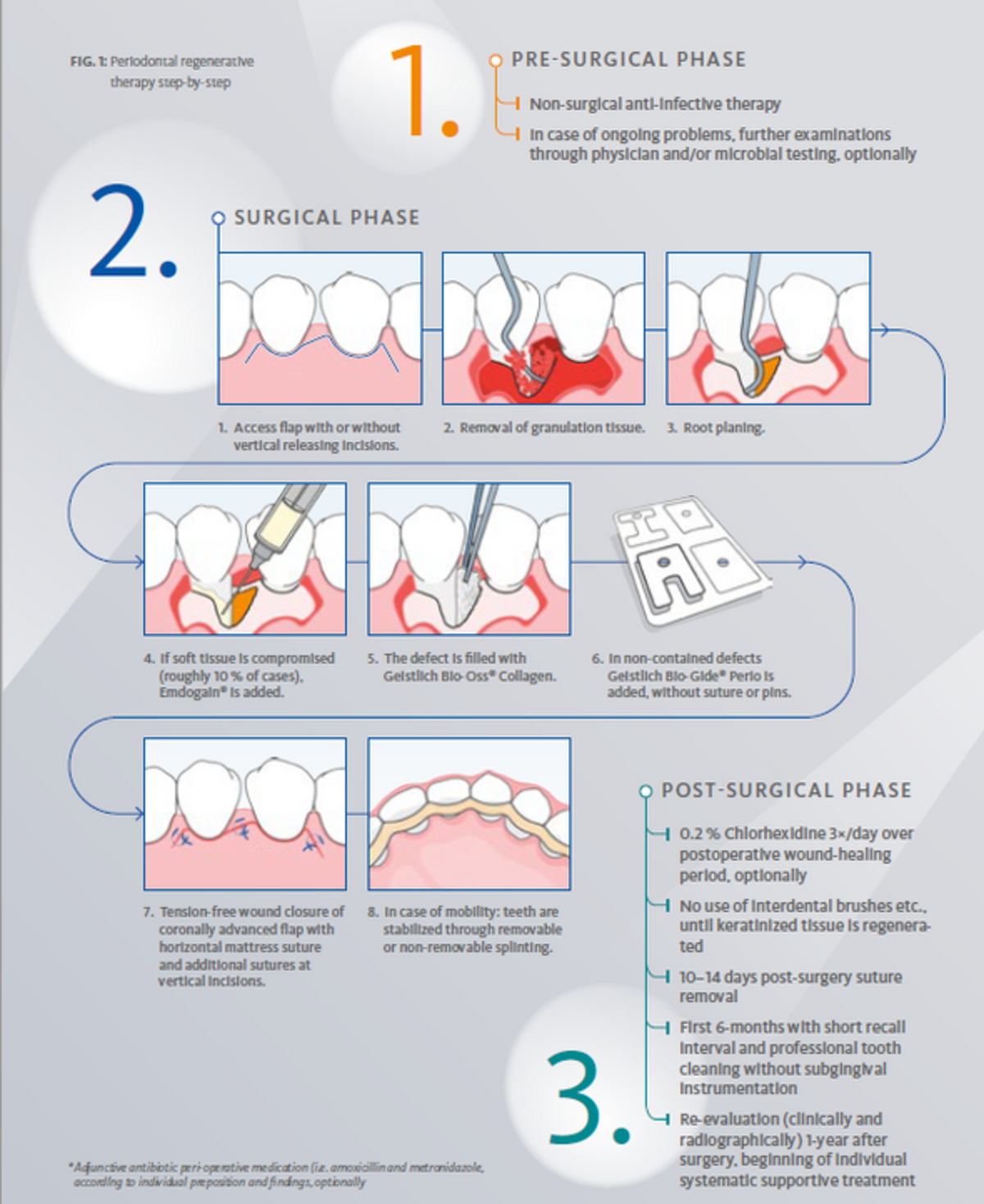
We analyzed 1008 teeth in 176 patients over ten years. All patients were treated according to our standard algorithm (Fig. 1). Despite the range of impairments in a normal patient population, we had the same treatment success as shown in the prospective studies. Radiographic bone fill was 3.8 mm after one year and remained stable for up to ten years. You might compare this to the amount of bone gain with open flap debridement alone which is about 0.95 mm.4 A higher amount of bone gain was achieved in deep defects, and probing pocket depths were significantly reduced and remained shallow over the observation period.
Some dentists find regenerative periodontal therapy too unpredictable. Do you agree?
Not at all. Our daily experience and clinical studies show that the opposite is true. But you do have to learn the right way to go about it. Young dentists often lack proper surgical training and must catch up with additional learning. This is demanding for the beginners, but without a very good education, nothing works out.
You also investigated how patients perceive the outcome of periodontal therapy.5 Which factor was most important for satisfaction?
It’s important to bear in mind: that patients come to us because they have complaints, like bleeding gums, a bad taste in their mouth or loose teeth. They never ask us to “fill their bony defects.” They want to be healthy again. If this can be achieved, they accept small imperfections, for example, in esthetics, that sometimes cannot be fully achieved.
So, esthetics aren’t the main concern?
No, they’re not. But depening on the patient, the esthetic outcome can still be very important. Everyone wants to be able to laugh without worries. Nobody wants to have to hide a smile behind their hand. And we can achieve this good esthetic result with regenerative periodontics.
Or let’s rather say regenerative periodontology is the first step toward a very good esthetic result, because in case of high esthetic demands, further treatments such as soft tissue plastic surgery or orthodontics are probably also needed.
In your publication patients were more satisfied after regenerative therapy compared with scaling and root planing or open flap debridement.5 Why?
They felt regenerative treatment had been very successful, although they started out from a very difficult situation.
Scaling and root planing (SRP) is easier to perform, but it leads to disease recurrence far more frequently than regenerative therapy. And open flap debridement (OFD) causes a gum recession. The consequences are sensitive teeth, poorer esthetics and more difficult oral hygiene – all of which may cause patient dissatisfaction.

Patients must be highly compliant for many years. Is there a critical point when the motivation becomes lower and patients must be re-motivated?
After about three years the process of regeneration is completed, a new status quo is reached. Then there is a risk that patients will become overconfident and too optimistic and, therefore, less thorough with their oral hygiene. We have to remind them that periodontitis is a chronic disease requiring a high level of compliance and very good oral hygiene for life.
What specific steps do you take to re-motivate patients?
After five years we ascertain the radiographic status and discuss it at length with the patients. We discuss the prognosis for all their teeth and illustrate with the colors red, yellow and green. We stress what has been achieved, but we also share literature about relapse rates and emphasize: “You can’t sit back now.”
Are patients concerned about preserving teeth?
For most, yes. Natural teeth have many advantages. It’s easier to chew with natural teeth, and they are not as susceptible as implants to infectious disease.
Implant marketing advertisement is very positive, and some patients believe that implants last forever. But the prognosis for an implant is only about 12-years.6 We can preserve the patient's natural teeth that long, and for most, probably longer.
Although regenerative periodontal therapy might be complex, it is always more cost-effective than an implant.
Do patients follow your recommendations?
Usually they do. If something is financially impossible, you have to lower your goals. Then we might opt for a healthy situation with diminished esthetics, for example.
For patients with very high expectations, we follow periodontal therapy with orthodontics, because periodontal diseases are often accompanied by dislocation of the teeth. Restoring the correct tooth position and natural anatomy, including papillae, is the best way to prevent recurrence. Where there’s an intact papilla, plaque has a harder time invading the periodontal tissues. The results are wonderful, but given the time and therapy required, the treatment is much more expensive.
Your own treatment algorithm is based not only on scientific data, but also on cost-balance. How long have you been working with this algorithm?
The algorithm has been the same for many years. I plan therapy exclusively according to medical criteria and the cost plan is based on this. I’ve never worked for profit. The profit comes instead from the fact that a very satisfied patient recommends our practice to others.
References
- Bröseler F, et al.: J Clin Periodontol 2017; 44 : 520-9. (clinical study)
- Cortelini P & Tonetti MS.: Periodontol 2000 2015; 68(1): 282-307. (systematic review)
- Sculean A, et al.: Periodontol 2000 2015; 68(1): 182-216. (systematic review)
- Graziani F, et al.: J Clin Periodontol 2012; 39(2): 145-56. (systematic review)
- Franke M, et al.: Oral Health Prev Dent 2015; 13: 163-8. (clinical study)
- Derks J, et al.: J Dent Res 2016; 95(1): 43-9. (clinical study)
About the author

Manager Medical Communications
Geistlich Pharma