"Patient was told implants were not an option for him."


Does jawbone atrophy necessarily have to mean the patient has to wear a removable prosthesis for the rest of their life? Not at the Campbell Clinic, where patients are offered a 10-year guarantee after a sinus lift procedure and implant placement.
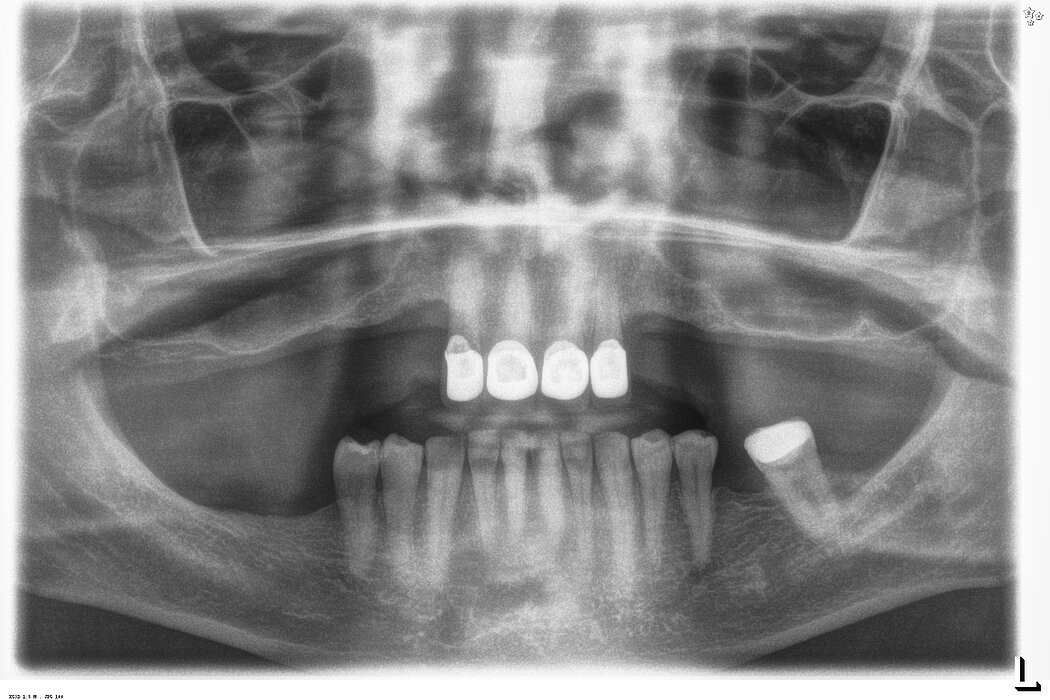
A 64-year-old patient came to the Campbell clinic in 2016 with a failing anterior bridge. He had a removable denture, which he could not use for more than a couple of hours at a time, as it irritated the soft tissue in the oral cavity.
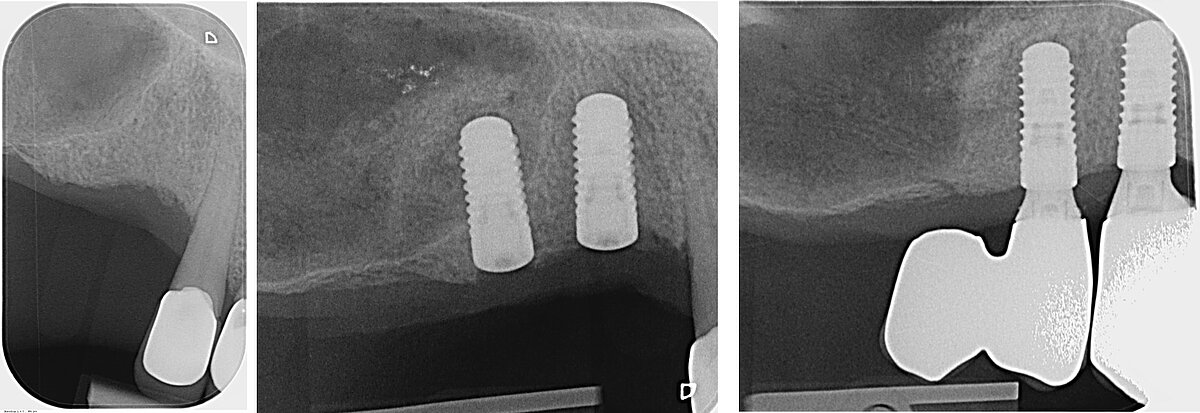
He had been told that fixed prostheses were not an option for him, as there was not enough bone available to support the implants.
Simultaneous sinus floor lift and posterior implant placement
We were certain we could increase the bone height in the 14 and 24 area (FDI system) using sinus floor lift with the lateral window technique and simultaneously placing two dental implants.
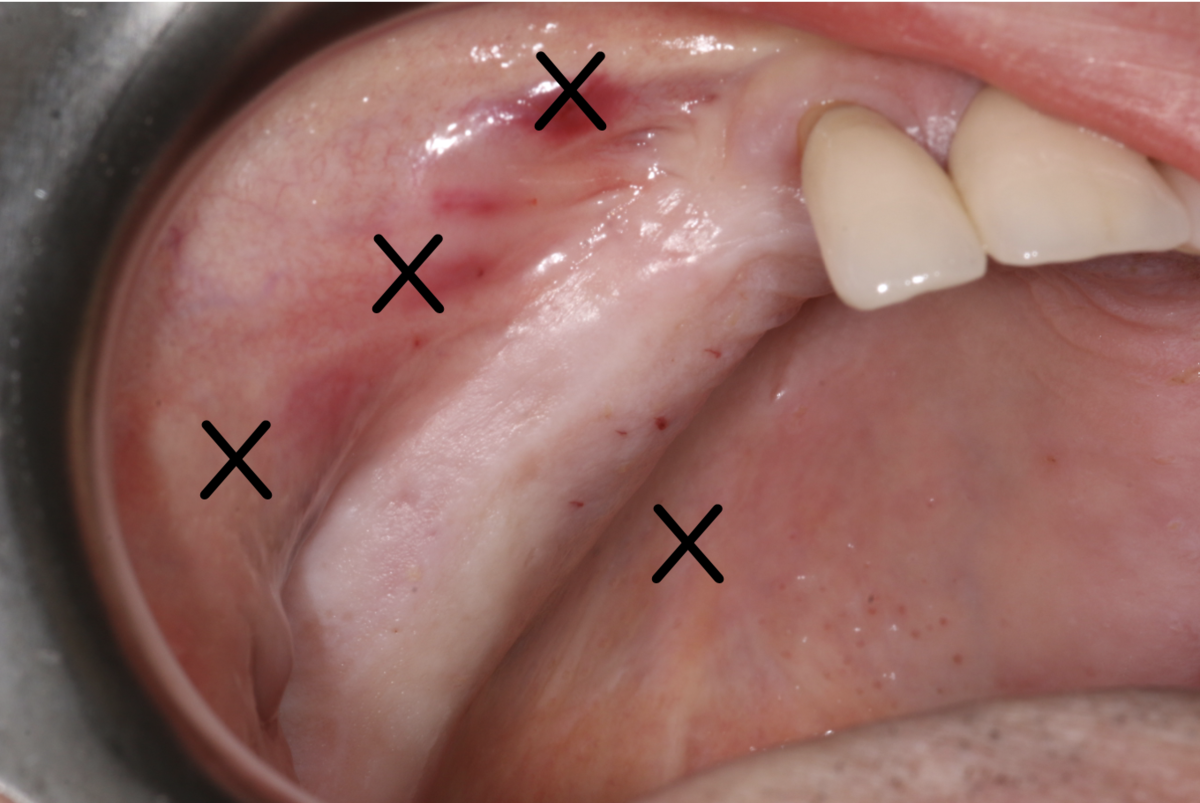
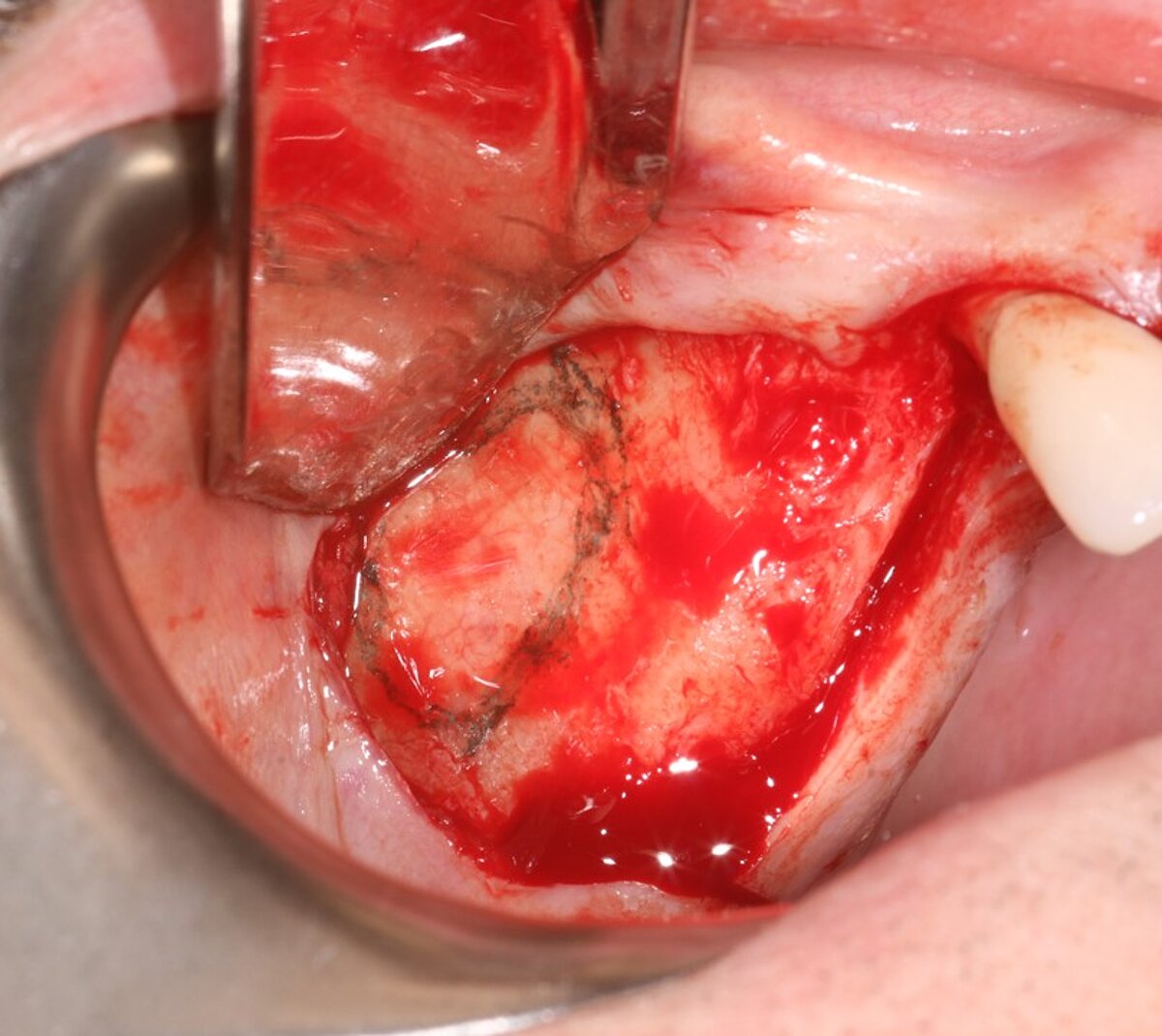
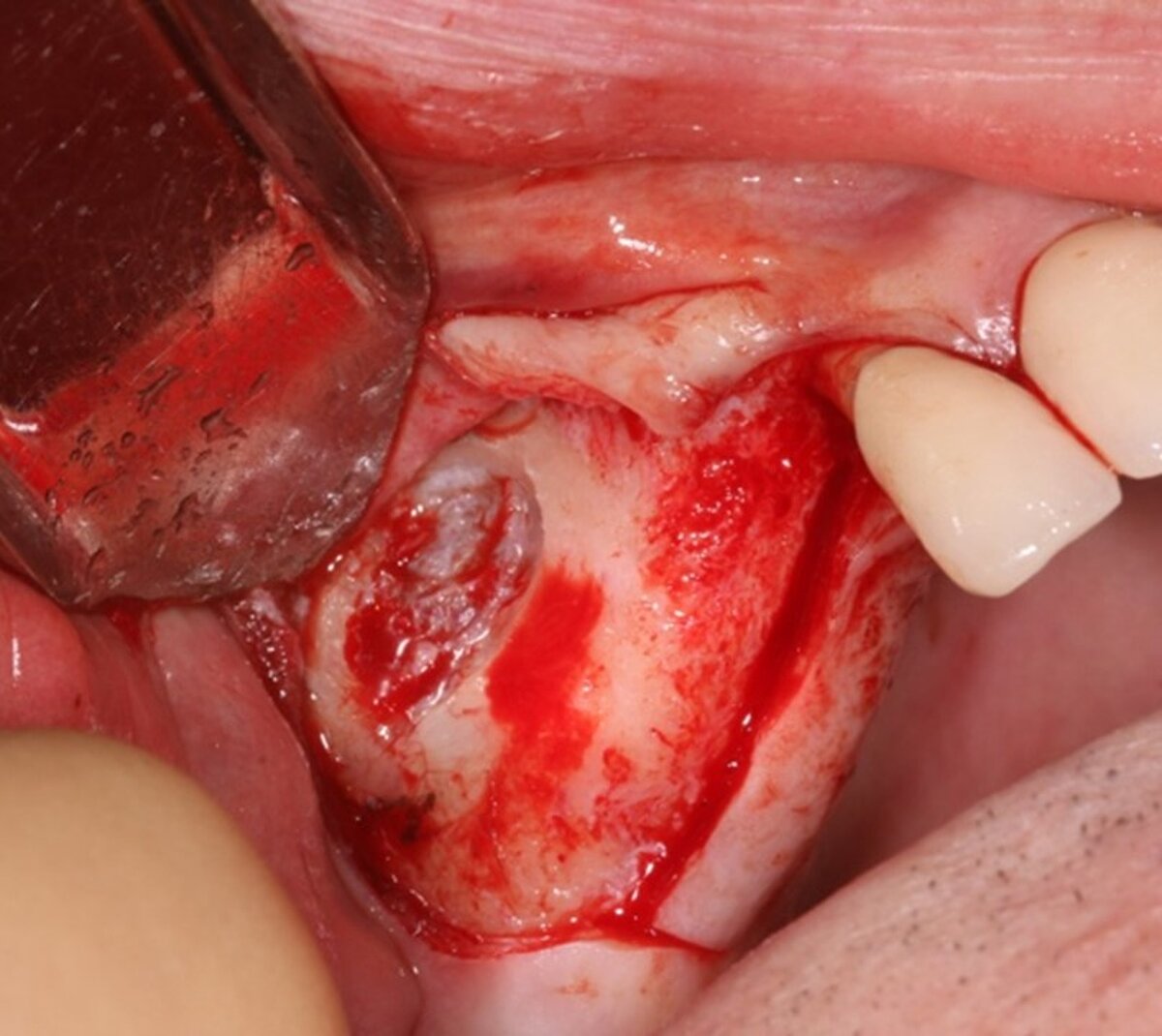
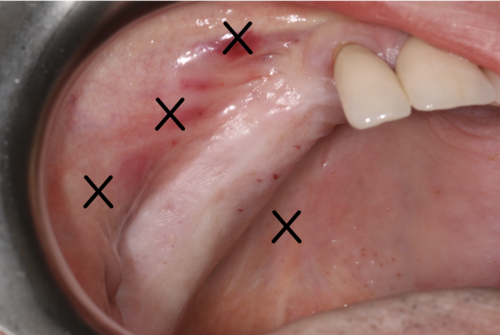
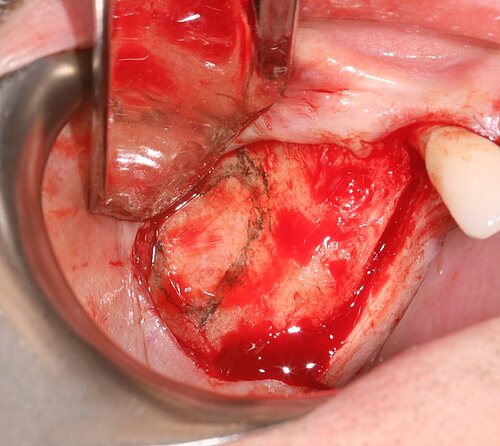
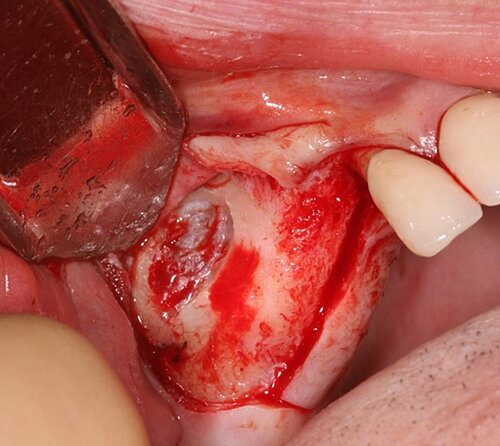
We used local anesthetic for vestibular infiltration which is higher and deeper than for straightforward implant placement (FIG 1). Mucoperiosteal full thickness flap was done and distal relieving incision, making sure it wouldn't cross the surgical area (FIG 2). Using a single-use bone harvester, SafeScraper® Twist, the autologous bone chips were collected (FIG 3). A lateral window area was marked for opening the window. Given the anatomical conditions, access was a straight line. It is always important to retain 4-5 mm of buccal bone and not to create a ledge. Rotatory or piezo instruments can be used to open the window (FIG 4). We started to release the membrane with small instruments (FIG 5) and moved to bigger ones as soon as possible.




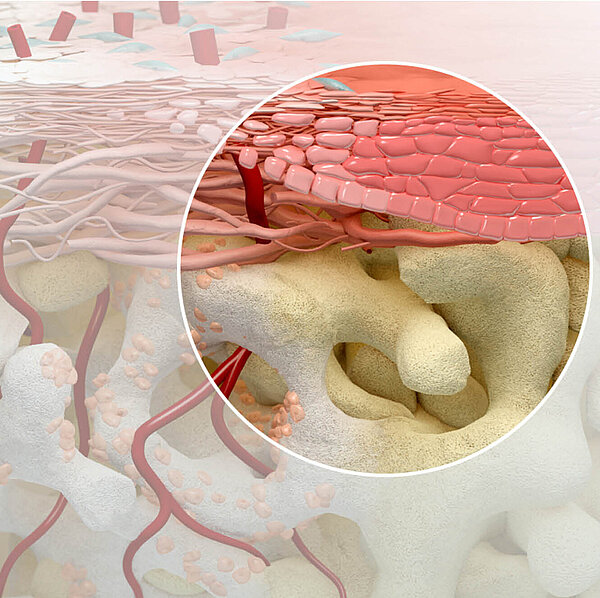
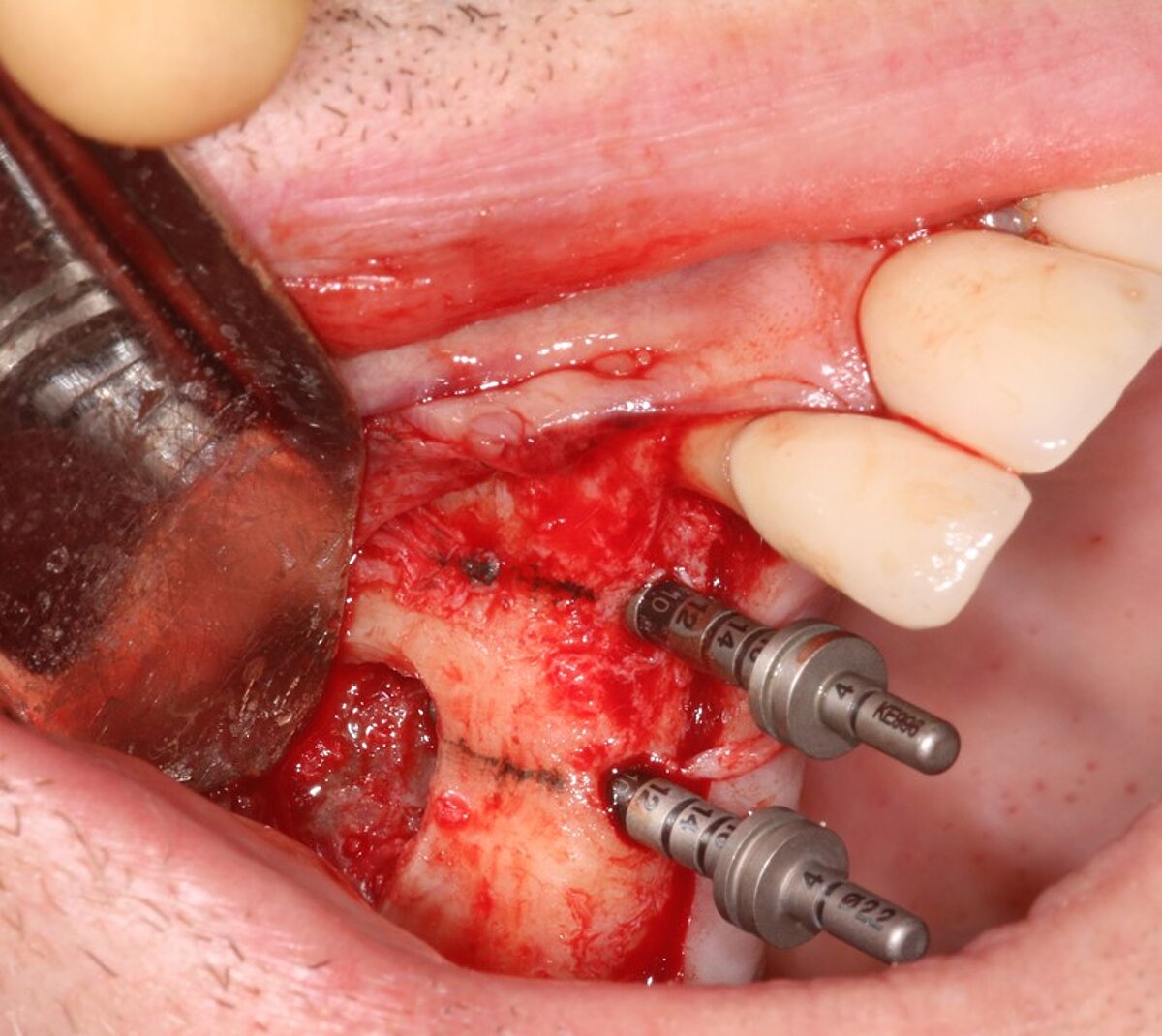
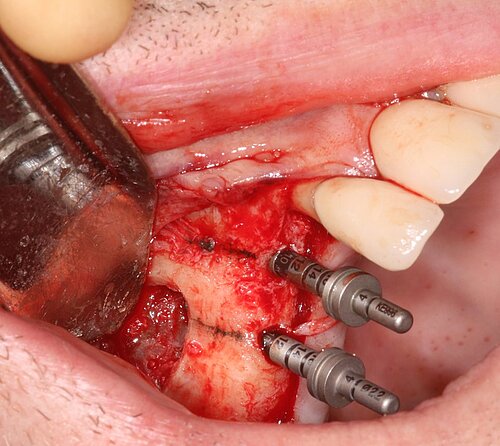
Once the membrane was mobile, implant osteotomies were prepared at 400 rpm, as the bone in the posterior maxilla is soft (FIG 6). Sinus graft was performed with a mix of 75% Geistlich Bio-Oss®, 1-2mm granule size, to work as a stable scaffold for new bone to be regenerated, and 25% autologous chips to provide more osteoconductivity, osteogenicity, and osteoinductivity (FIG 7).
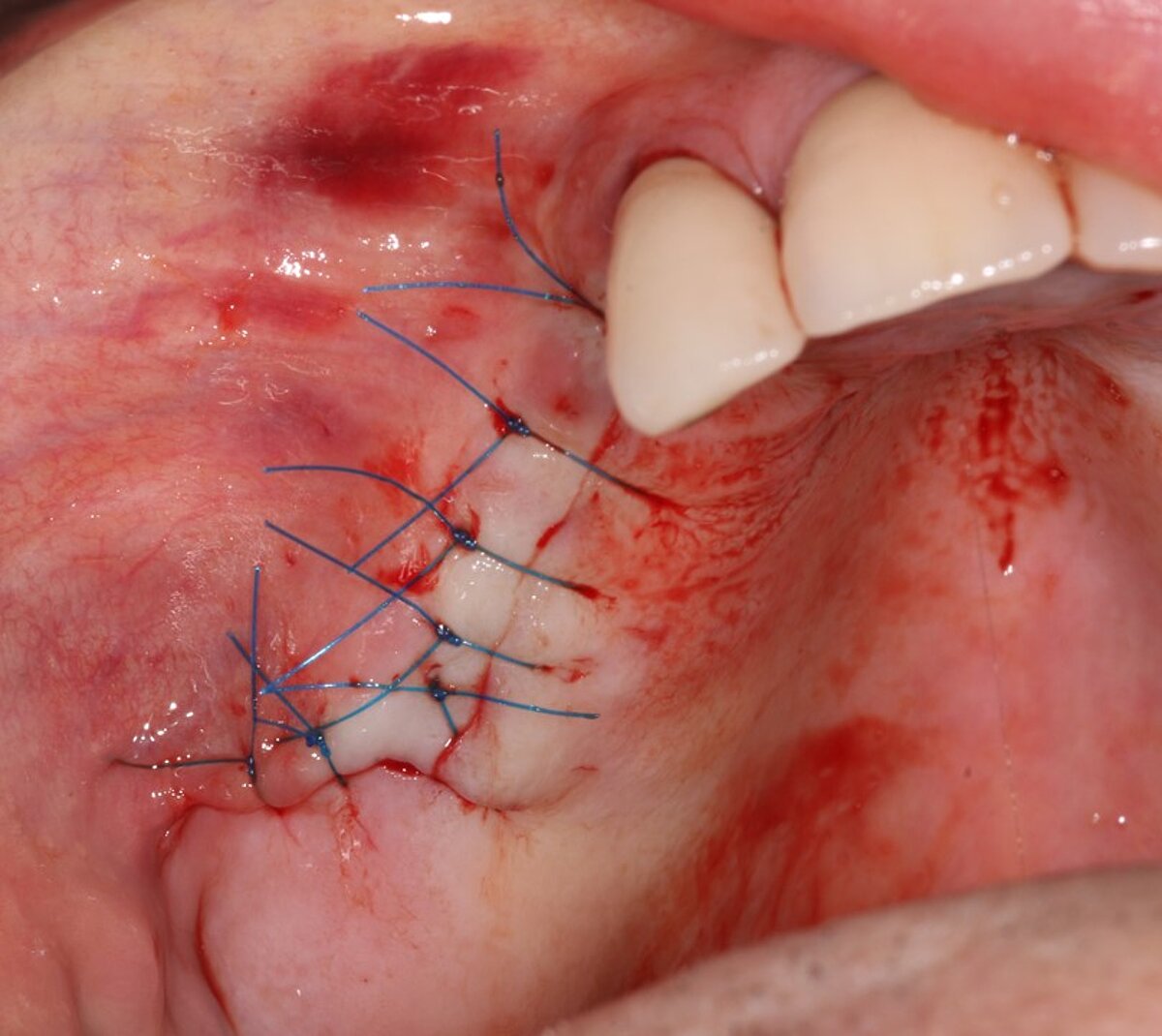
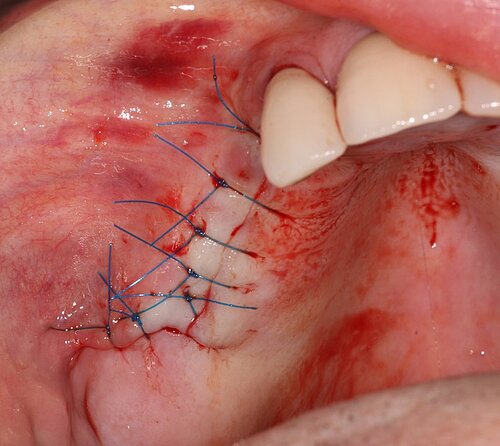
As the primary stability was good, implants were inserted in the pre-prepared osteotomy in the same surgery (FIG 8). We always measure the resonance frequency stability (implant stability quotient, ISQ) on insertion, and on exposure, e.g. eight weeks later and carry out restorative procedures if these have increased. We covered the lateral window with a double layer of Geistlich Bio-Gide® to give the grafted area stability and protect it from soft tissue growth (Fig 9). Also, periosteal relieving incision was done to close the flap tension free (FIG 10).






Ten weeks later, the fixed prosthesis was placed. The upper left quadrant was restored in the same way which allowed the patient to completely get rid of his uncomfortable removable prosthesis and have a restoration with adequate posterior support.
Final remarks
The treatment was completed in a total of twelve weeks from start to finish and provided a predictable fixed solution in an area the patient thought was unrestorable, and in a quick turnaround time, making the full procedure easy and comfortable for the patient. He was delighted with the results. We have been routinely placing implants in the practice for over 20 years and offered patients a 10-year guarantee, based on our long-term results which are systematically and carefully monitored. We also use Geistlich biomaterials whenever hard and soft tissue regeneration is required, as we trust they are evidence-based and scientifically proven.
About the authors

Campbell Clinic & The Campbell Academy Director, Nottingham

Campbell Clinic Surgeon
Campbell Academy Faculty Member