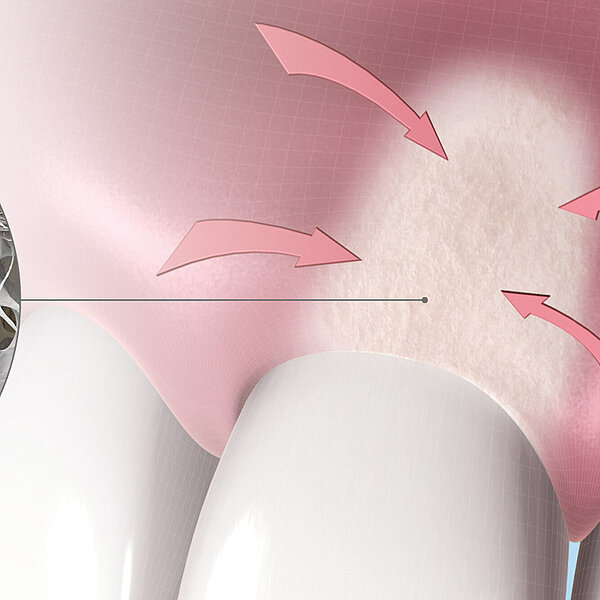
Ridge preservation reduces the need for GBR at implant placement



What is the rationale for Ridge Preservation and socket sealing before early implant placement? Why should the extraction socket not be left to heal on its own? A randomized clinical trial with 75 patients answers these questions.
You have recently published an article which compares Ridge Preservation and spontaneous healing before early implant placement. How did the results differ for different treatment modalities?
Seventy‐five patients underwent early implant placement after tooth extraction and were evaluated. The ridge preservation groups showed less horizontal bone resorption than the control group. Moreover, the necessity of GBR at implant placement was significantly lower in the ridge preservation group.
What protocol do you use?
A flapless extraction procedure was performed using periotome, elevators, and forceps. If needed, a drill was used to remove the tooth in multiple pieces. After extraction, any existing granulation tissue was removed, and the socket was rinsed with sterile saline. The soft tissue borders of the alveolus were de‐epithelialized using a rotating diamond bur. A biomaterial was placed within the socket up to the level of the lingual/palatal bone plate. A collagen matrix or palatal graft was placed on top and sutured to the gingival margins of the socket with 4 to 6 interrupted sutures. Implants were placed after 8 weeks.
Then you always seal the socket with either a palatal punch graft or collagen matrix. Does the choice of sealing material change the clinical outcome? Which one did you prefer?
For this study we used a palatal punch graft and a collagen matrix (Geistlich Mucograft® Seal). Regarding the hard and soft tissue changes, no significant differences were found. Patients with sockets sealed with the collagen matrix experienced less pain than those with the palatal punch graft, one week after tooth extraction.
We preferred ridge preservation with a collagen matrix instead of a palatal graft because it is definitely more convenient for the patient and saves an extra surgical procedure and therefore patient morbidity.
Is there any indication in which you don’t fill the socket after extraction?
In the esthetic zone, we perform socket preservation if dental implant placement is expected and immediate implant placement is not feasible. We do not perform ridge preservation in medically compromised patients with a contra-indication for implantology.
Do you suggest this protocol to implant surgeon starters?
For starting surgeons placing implants early after alveolar ridge preservation, this might be more difficult than late implant placement after ARP. The augmented biomaterial is still quite soft at early implant placement and some particles are easily displaced during drilling of the bone, resulting in the need for additional augmentation. For surgeon starters, we would advise ARP with late implant placement or immediate implant placement in selected cases.
Reference
1. Jonker BP, et al.: Clin Oral Impl Res. 2021;32:123–33 (clinical study)
About the authors

Manager Medical Communications
Geistlich Pharma AG

Department of Oral & Maxillofacial Surgery,
Special Dental Care and Orthodontics,
Erasmus University Medical Center,
Rotterdam, The Netherlands

Department of Oral & Maxillofacial Surgery,
Catharina Hospital Eindhoven, Eindhoven,
The Netherlands